
Key Points:
- Nutrient deficiencies can drive appetite disturbances, sugar cravings, and binge eating, making targeted supplementation essential for recovery.
- Digestive support (enzymes, probiotics) and trace minerals (zinc, magnesium, chromium) help the body absorb nutrients and regulate metabolism, mood, and appetite.
- B vitamins, folate, inositol, and essential fatty acids support neurotransmitter balance, mood stabilization, and insulin sensitivity, reducing cravings.
- Anti-inflammatory and metabolic supplements like curcumin and gymnema can decrease inflammation, improve blood sugar control, and suppress sugar cravings.
- Individualized supplementation guided by a healthcare professional, based on metabolic and nutrient testing, is key to restoring appetite control and improving eating disorder outcomes.
Nutrient deficiencies often contribute to the stranglehold of appetite disturbances and can intensify devastating patterns of disordered eating. When your body is provided with the right nutrients, you are better equipped to achieve success and regain control over your appetite, cravings and binge eating.
Working with a qualified healthcare practitioner to explore the latest nutritional psychiatry protocols in identifying personal nutrient imbalances and implementing a unique supplementation plan can be a powerful step in recovery from binge eating disorders.
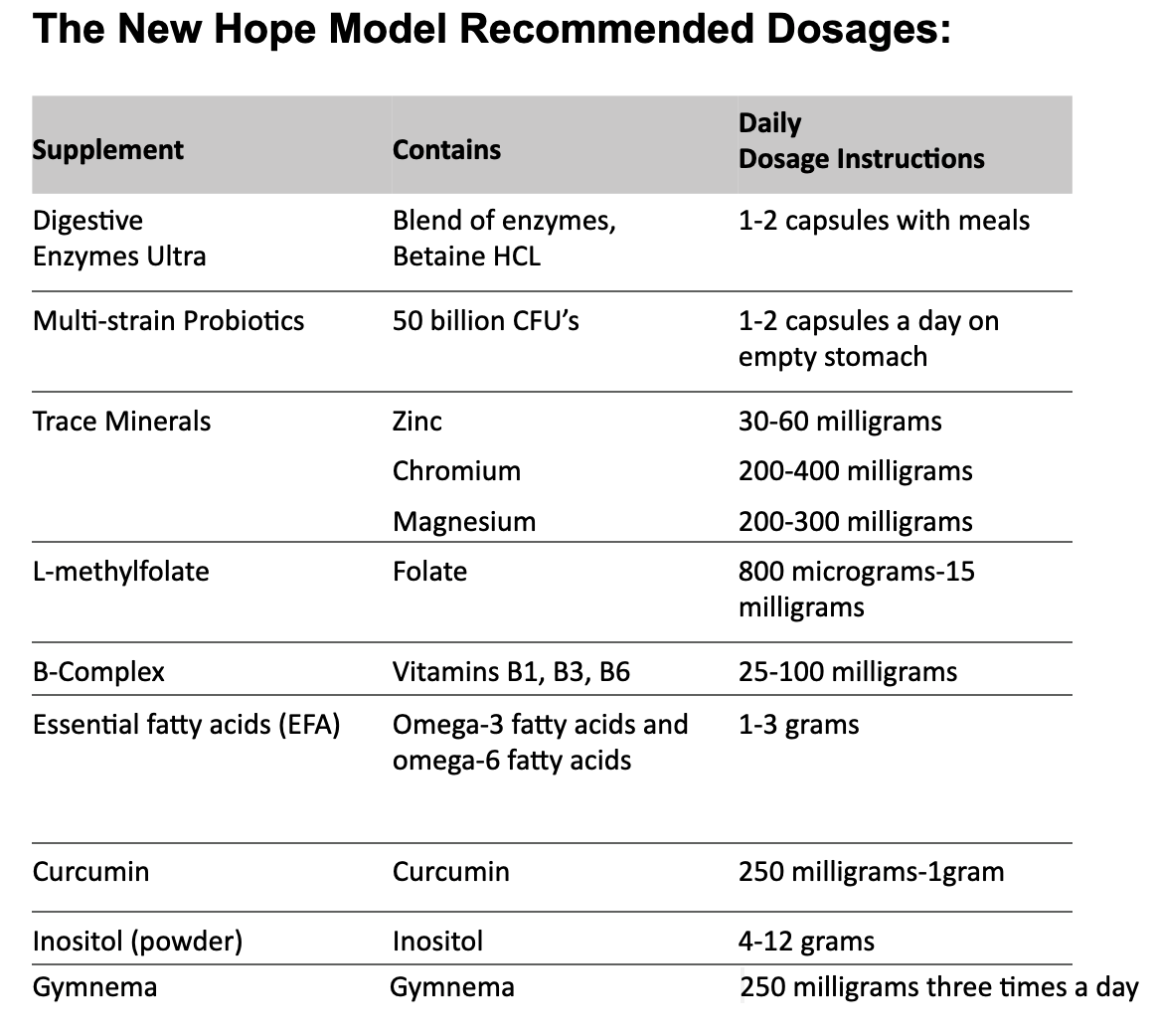
Over many years of clinical experience, I have found specific nutritional supplements invaluable in the treatment of eating disorders. That’s why I created the New Hope model in my book, Integrative Medicine for Binge Eating. The model incorporates 9 nutrients which I believe are essential to helping patients regain control over their appetite and lives when suffering from the debilitating disorder of binge eating.
1. Digestive Enzymes
Recovery from disordered eating depends on a healthy digestive system. I often see patients who eat healthy diets consisting of organic foods and adequate protein, whose blood work nevertheless reveals that they are, in fact, malnourished. Nutritional status is not based on what you eat. Instead, it depends upon your ability to digest and absorb nutrients from food.
The stomach chemically and mechanically transforms food into a liquid mixture, composed of partially digested food, water, digestive enzymes, and hydrochloric acid (HCL). The extremely acidic nature of HCL is essential for proper digestion, as it helps break down protein, absorb vitamins and minerals, and communicate to the brain that you are full. In other words, hydrochloric acid is good for digestion.
Most vitamins and minerals are also absorbed in the small intestine. Therefore, the health of the small intestine is a critical determining factor in nutrient absorption.
2. Probiotics
Studies with overweight patients have shown probiotic supplementation can produce a significant decrease in sugar cravings in as few as four days. Probiotics contain plentiful amounts of bacteria that can “seed” the intestines and promote the multiplication of these helpful organisms.
Probiotic-containing foods include fermented foods such as yogurt and kefir, sauerkraut, kimchi, tempeh, miso, and kombucha. Probiotic supplements, however, offer much more concentrated doses of bacteria – sometimes numbering in the billions – and are therefore much more effective than probiotic-containing foods at restoring the intestinal microbiota.
Scientific evidence suggests that the quality and quantity of microorganisms in the gut in both humans and animals are different in the lean than in the overweight, citing a relationship between bacteria and disordered eating behavior. Research has shown that overweight individuals have much greater amounts of Firmicutes and lesser amounts of Bacteroidetes than their lean counterparts. But when these overweight individuals lose weight, the proportions of bacteria shift and begin to resemble those of lean people.
3. Trace Minerals: Zinc, Magnesium, and Chromium
Numerous trace minerals are essential for human health and optimal brain function, and three of these are particularly helpful for the treatment of eating disturbances.
The mineral zinc plays important roles in growth and development, neurologic function, the immune response, reproduction, and neurotransmitter synthesis. Vital chemical reactions involving nearly one hundred different enzymes, including digestive enzymes, cannot be catalyzed without zinc. Zinc is also critical to our senses of taste and smell, bone growth, the production of proteins, DNA synthesis, cell division, and wound healing.
Low zinc status is also related to depression. Research has shown that people with major depression have zinc levels that are twelve to sixteen percent lower than those who are not depressed.
Inadequate chromium levels result in carbohydrate cravings, impaired glucose tolerance, hypoglycemia, and depression. Chromium is an essential part of glucose tolerance factor (GTF), a compound that helps insulin move blood sugar into the cells. Chromium works with the insulin receptors on the cells, helping “open the doors” so that glucose can enter. And even though the body contains a very small amount of chromium, when its stores become depleted, the effectiveness of insulin and the body’s ability to handle glucose can markedly decrease. Poorly controlled glucose levels, in turn, can result in sugar or carbohydrate cravings and an increase in hunger.
Magnesium plays a vital role in many of the body’s metabolic processes, including the conversion of protein, fat, and carbohydrates into energy. Moreover, magnesium is critical for the proper functioning of over three hundred enzymes, including those necessary for the synthesis of neurotransmitters such as serotonin. Common symptoms associated with magnesium deficiency include headaches, constipation, insomnia, premenstrual syndrome (PMS), fatigue, anxiety, insulin resistance, and sugar cravings.
Magnesium deficiency can also cause psychological conditions including depression, irritability, and anxiety. Research studies have shown that oral magnesium treatment can be particularly effective in treating major depression.
4. B Vitamins
The B vitamins are important for normalizing eating patterns, as they help stabilize blood glucose levels. The vitamins that make up the B complex include thiamin, riboflavin, niacin, B6, B12, pantothenic acid, inositol, biotin, folic acid, and others that work together to convert carbohydrates into glucose, which means they help provide energy, decrease sugar cravings, fight fatigue, and ease hypoglycemia-related mood swings.
These vitamins are also important in preventing depression. For example, at least four different double-blind studies have found that boosting thiamin levels lifts the mood of study participants. Additionally, vitamin B6 supplementation has been shown to stabilize mood in depressed patients; folic acid supplements given to depressed patients shortened the patients’ recovery time; and mood and memory has improved in patients given B12 supplements.
The B vitamins most important to the regulation of appetite include vitamin B6, vitamin B12, inositol, and folate. They can be taken as single supplements or, in many cases, taken together in the form of a B complex.
5. Folate (L-methylfolate)
The B vitamin folate, also referred to as folic acid, is crucial to the growth and maintenance of all cells as well as the synthesis of DNA. It markedly affects the production of all new proteins, especially proteins with a fast turnover rate such as those found in red blood cells, the cells lining the digestive tract, and the cells of a growing fetus. Low folate levels can cause anemia, gastrointestinal upset, and major defects in the fetal brain and spine known as neural tube defects. Folate-deficient individuals can also develop elevated blood levels of homocysteine, a risk factor for cardiovascular disease and Alzheimer’s disease.
Folate assists in the manufacture of serotonin, dopamine, and norepinephrine, and deficiencies are common in people with depression. Research has shown folate and depression severity to be inversely correlated; in other words, lower folate levels are associated with more severe depression.
Numerous studies have also found that depressed people who have low folate levels respond more poorly to antidepressant treatment and relapse more frequently than others. Higher folate levels, on the other hand, are linked to lower depression risk and severity. Taking folate supplements seems to also enhance the effects of antidepressants and relieve depression more effectively than simply taking antidepressants alone. However, those with a specific biochemical makeup may respond best to a form of the vitamin called L-methylfolate.
6. Essential Fatty Acids
There are two families of EFAs: the omega-3s, which are found primarily in fish or fish oil and can be created in the body from flax oil; and the omega-6s, which are found primarily in vegetable oils and grains. Growth and development, brain and nerve function, the control of inflammation, and the regulation of metabolism all depend on sufficient amounts of omega-3s being present for use within the body.
Omega-6 intake has risen steadily over the past century due to the increasing prevalence and usage of plant oils – including corn, cottonseed, safflower, and sunflower oils – in the western diet. High concentrations of omega-6s ‘crowd out’ omega-3s, which means that more and more people worldwide are now consuming diets that provide too many omega-6s and too few omega-3s.
An EFA deficiency or a skewing of the omega-6 : omega-3 ratio can contribute to depression, obesity, and blood sugar abnormalities, all of which can affect eating habits and appetite. People who follow restrictive diets or who simply cut back drastically on fat intake may find themselves deficient in EFAs.
7. Curcumin
Recent studies reveal the healing powers of curcumin, a component of the common household spice turmeric. With antioxidant and anti-inflammatory properties, curcumin imitates the antidepressant actions of the prescription drugs fluoxetine and imipramine – without any of the side effects.
It has also been touted as an anti-obesity agent for its ability to reduce body fat and inhibit weight gain. A study published in the Journal of Nutrition reported that mice fed a high-fat diet along with supplemental curcumin had decreased weight gain and lowered cholesterol levels.
Curcumin has been shown to improve depressed mood, sleep disturbances, and fatigue. People with depression tend to have increased inflammation and decreased neurogenesis, both of which can be restored to healthy levels by curcumin.
8. Inositol
Inositol, also known as vitamin B8, is responsible for forming healthy cell membranes and maintaining nutrient transfer between cells. Inositol is converted into a substance that regulates the action of serotonin. Restoring normal levels of this vitamin may thus help alleviate psychiatric symptoms, including depression, feelings of panic, and obsessive thoughts.
Present in the tissues of the brain, nerves, muscles, bones, heart, and reproductive system, inositol is a precursor to several “signaling” molecules that tell cells how to behave. Inositol enhances insulin sensitivity, which can produce more energy, reduce cravings, and suppress the desire to binge. It also participates in the action of serotonin.
Inositol has been effective in treating many of the same psychiatric disorders that are linked to eating disorders and responsive to SSRIs, including depression, anxiety, and obsessive-compulsive disorder.
9. Gymnema
Gymnema sylvestre is a traditional Ayurvedic herb that is native to central and western India, Africa and Australia. Its Hindi name, “gurmar,” means “destroyer of sugar.” Commonly found in most health food stores the form of tea, it is considered to have antidiabetic properties and is used to control obesity. When the leaves are chewed, it interferes with the ability to taste sweetness. Gymnema can be helpful for suppressing sugar cravings.
The active property of gymnema is gymnemic acid, which delays glucose absorption in the blood. Because the molecular structure of gymnemic acid is similar to glucose, it can help curb sugar cravings by filling in the receptor locations of sweet taste buds. Though more research is needed, gymnema may be an alternative medicine to treat sugar cravings due to its efficacy in blocking sugar binding sites, and by preventing sugar molecules from accumulating in the body.
Takeaway
In my decades of experience treating patients with eating disorders, I have found that specific nutrient supplements are amazingly effective in assisting patients. Rather than treating symptoms alone, the most effective treatment targets nutritional and metabolic imbalances that are interfering with your body’s ability to regulate appetite. Once balance is restored, the symptoms often diminish or even disappear.
I suggest that you work with a healthcare provider familiar with biochemical individuality to create an individualized supplement program based on the results of your metabolic tests. Don’t try to figure it out yourself, as overloading on supplements or taking supplements you don’t need can be both expensive and frustrating, and lead to another journey toward failure.
Taking supplements to correct nutritional deficiencies is the foundation in the New Hope model for restoring appetite control. For more information on the model, please refer to my book that fully explores the subject, Integrative Medicine for Binge Eating.
If you are a patient seeking more holistic care, check out the Psychiatry Redefined Preferred Providers Directory. All of the providers in our directory have been trained by Psychiatry Redefined.
Ready to learn breakthrough nutritional and functional strategies to help your patients? Enroll now in the comprehensive online Fellowship in Functional Psychiatry. Book a private call to learn more!
References
- Abou-Saleh MT, Coppen A. Serum and red blood cell folate in depression. Acta Psychiatr Scand. 1989;80(1):78-82.
- Barragan-Rodriguez L, Rodriguez-Moran M, Guerreo-Romero F. Efficacy and safety of oral magnesium supplementation in the treatment of depression in the elderly with type 2 diabetes: a randomized, equivalent trial. Magnesium Res. 2008;21(4):218-223.
- Benjamin J, Levine J, Fux M, Aviv A, Levy D, Belmaker RH. Doubleblind, placebo-controlled, crossover trial of inositol treatment for panic disorder. Am J Psychiatry. 1995;152(7):1084-1086.
- Beydoun MA, Fanelli Kuczmarski MT, Beydoun HA et al. The sex-specific role of plasma folate in mediating the association of dietary quality with depressive symptoms. J Nutr. 2010;140(2):338-347.
- Ciacci C, Peluso G, Iannoni E et al. L-carnitine in the treatment of fatigue in adult celiac disease patients: a pilot study. Dig Liver Dis. 2007;39(10):922-928.
- Colodny L, Hoffman RL. Inositol—Clinical applications for exogenous use. Altern Med Rev. 1998;3(6):432-447.
- Coppen A. Bailey J. Enhancement of the antidepressant action of fluoxetine by folic acid: a randomized, placebo-controlled trial. J Affect Disord. 2000;60(2):121-130.
- Cruciani RA, Dvorkin E, Homel P et al. Safety, tolerability and symptom outcomes associated with L-carnitine supplementation in patients with cancer, fatigue and carnitine deficiency: a phase I/II study. J Pain Symptom Manage. 2006;32(6):551-559.
- Davidson JR, Abraham K, Connor KM, McLeod MN. Effectiveness of chromium in atypical depression: a placebo-controlled trial. Biol Psychiatry. 2003;53(3):261-264.
- Docherty JP, Sack DA, Roffman M, Finch M, Komorowski JR. A double-blind, placebo-controlled, exploratory trial of chromium picolinate in atypical depression: effect on carbohydrate craving. J Psychiatr Pract. 2005;11(5):302-314.
- Eby GA, Eby KL. Rapid recovery from major depression using magnesium treatment. Med Hypotheses. 2006;67(2):362-370.
- Fava M, Mischoulon D. Folate in depression: Efficacy, safety differences in formulations and clinical issues. J Clin Psychiatry. 2009;70(Suppl 5):12-17.
- Fava M, Borus JS, Alpert JE, Nierenberg AA, Rosenbaum JF, Bottiglieri T. Folate, vitamin B12 and homocysteine in major depressive disorder. Am J Psychiatry. 1997;154(3):426-428.
- Ford ES, Mokdad AH. Dietary magnesium intake in a national sample of U.S. adults. J Nutr. 2003;133(9):2879-2882.
- Fux M, Benjamin J, Belmaker RH. Inositol versus placebo augmentation of serotonin reuptake inhibitors in the treatment of obsessivecompulsive disorder: a double-blind cross-over study. Int J Neuropsychopharmacol. 1999;2(3):193-195.
- Hansen CR Jr., Malecha M, Mackenzie TB, Kroll J. Copper and zinc deficiencies in association with depression and neurological findings. Biol Psychiatry. 1983;18(3):395-401.
- Hintikka J, Tolmunen T, Tanskanen A, Viinamäki H. High vitamin B12 level and good treatment outcome may be associated in major depressive disorder. BMC Psychiatry. 2003; 3:17.
- Jacka FN, Overland S, Stewart R, Tell GS, Bjelland I, Mykletun A. Association between magnesium intake and depression and anxiety in community-dwelling adults: the Hordaland health study. Aust N Z J Psychiatry. 2009;43(1):45-52.
- Kishi T, Watanabe T, Folkers K. Bioenergetics in clinical medicine XV. Inhibition of coenzyme Q10-enzymes by clinically used adrenergic blockers of beta-receptors. Res Commun Mol Pathol Pharmacol. 1977;17(1):157-164.
- Levenson CW. Zinc: the new antidepressant? Nutr Rev. 2006;64(1):39-42.
- Maes M, D’Haese PC, Scharpé S, D’Hondt P, Cosyns P, De Broe ME. Hypozincemia in depression. J Affect Disord. 1994;31(2):135-140.
- Maes M, Vandoolaeghe E, Neels, H et al. Lower serum zinc in major depression is a sensitive marker of treatment resistance of the immune/inflammatory response in that illness. Biol Psychiatry. 1997;42(5):349-358.
- Malaguarnera M, Cammalleri L, Gargante MP, Vacante M, Colonna V, Motta M. L-carnitine treatment reduces severity of physical and mental fatigue and increases cognitive functions in centenarians: a randomized and controlled clinical trial. Am J Clin Nutr. 2007;86(6):1738-1744.
- Mamalakis G, Tornaritis M, Kafatos A. Depression and adipose essential polyunsaturated fatty acids. Prostaglandins Leukot Essent Fatty Acids. 2002;67(5):311-318.
- McLeod MN, Golden RN. Chromium treatment of depression. Int J Neuropsychopharmacol. 2000;3(4):311-314.
- McLoughlin IJ, Hodge JS. Zinc in depressive disorder. Acta Psychiatr Scand. 1990;82(6):451-453.
- Milaneschi Y, Shardell M, Corsi AM et al. Serum 25-hydroxyvitamin D and depressive symptoms in older women and men. J Clin Endrocrinol Metab. 2010;95(7):3225-3233.
- Mizuno K, Tanaka M, Nozaki S et al. Antifatigue effects of coenzyme Q10 during physical fatigue. Nutrition. 2004;24(4):293-299.
- Morris MC, Evans DA, Bienias JL et al. Dietary folate and vitamin B12 intake and cognitive decline among community-dwelling older persons. Arch Neurol. 2005;62(4):641-645.
- Morris MS, Jacques PF, Rosenberg IH, Selhub J. Folate and vitamin B-12 status in relation to anemia, macrocytosis and cognitive impairment in older Americans in the age of folic acid fortification. Am J Clin Nutr. 2007;85(1):193-200.
- Narang RL, Gupta KR, Narang AP, Singh R. Levels of copper and zinc in depression. Indian J Physiol Pharmacol. 1991;35(4):272-274.
- Nowak G, Siwek M, Dudek D, Zieba A, Pilc A. Effect of zinc supplementation on antidepressant therapy in unipolar depression: a preliminary placebo-controlled trial. Pol J Pharmacol. 2003;55(6):1143-1147.
- Nowak G, Szewczyk B, Pilc A. Zinc and depression. An update. Pharmacol Rep. 2005;57(6):713-718.
- Otto SJ, de Groot RH, Hornstra G. Increased risk of postpartum depressive symptoms is associated with slower normalization after pregnancy of the functional docosahexaenoic acid status. Prostaglandins Leukot Essent Fatty Acids. 2003;69(4):237-243.
- Palatnik A, Frolov K, Fux M, Benjamin J. Double-blind, controlled, crossover trial of inositol versus fluvoxamine for the treatment of panic disorder. J Clin Psychopharmacol. 2001;21(3):335-339.
- Papakostas GI, Petersen T, Mischoulon D et al. Serum folate, vitamin B12 and homocysteine in major depressive disorder, Part 2: predictors of relapse during the continuation phase of pharmacotherapy. J Clin Psychiatry. 2004;65(8):1096-1098.
- Plioplys AV, Plioplys S. Amantadine and L-carnitine treatment of chronic fatigue syndrome. Neuropsychobiology. 1997;35(1):16-23.
- Preuss G, Anderson RA. Chromium update: examining recent literature 1997-1998. Curr Opin Clin Nutr Metab Care. 1998;1(6):509-512.
- Russ CS, Chrisley BM, Hendricks TA. Vitamin B6 status of depressed and obsessive-compulsive patients. Nutr Rep Int. 1983;27(4):867-873.
- Sawada T, Yokoi K. Effect of zinc supplementation on mood states in young women: a pilot study. Eur J Clin Nutr. 2010;64(3):331-333.
- Siwek M, Dudek D, Paul IA et al. Zinc supplementation augments efficacy of imipramine in treatment resistant patients: a double-blind, placebo-controlled study. J Affect Disord. 2009;118(1-3):187-195.
- Stewart JW, Harrison W, Quitkin F, Baker H. Low B6 levels in depressed outpatients. Biol Psychiatry. 1984;19(4):613-616.
- Sublette ME, Hibbeln JR, Galfalvy H, Oquendo MA, Mann JJ. Omega-3 polyunsaturated essential fatty acid status as a predictor of future suicide risk. Am J Psychiatry. 2006;163(6):1100-1102.
- Szewczyk B, Poleszak E, Sowa-Kućma M et al. Antidepressant activity of zinc and magnesium in view of the current hypotheses of antidepressant action. Pharmacol Rep. 2008;60(5):588-599.
- Tassabehji NM, Corniola RS, Alshingiti A, Levenson CW. Zinc deficiency induces depression-like symptoms in adult rats. Physiol Behav. 2008;95(3):365-369.
- Tiemeier H, van Tuijl HR, Hofman A, Meijer J, Kiliaan AJ, Breteler MM. Vitamin B12, folate and homocysteine in depression: the Rotterdam Study. Am J Psychiatry. 2002;159(12):2099-2101.
- Wójcik J, Dudek D, Schlegel-Zawadzka M et al. Antepartum/postpartum depressive symptoms and serum zinc and magnesium levels. Pharmacol Rep. 2006;58(4):571-576.
Photo Credits: Photo by Jane D. from Pexels